Edwards syndrome, Trisomy 18
Published: 18 Jun 2025
ICD9: 758.2 ICD10: Q91.3 ICD11: LD40.2
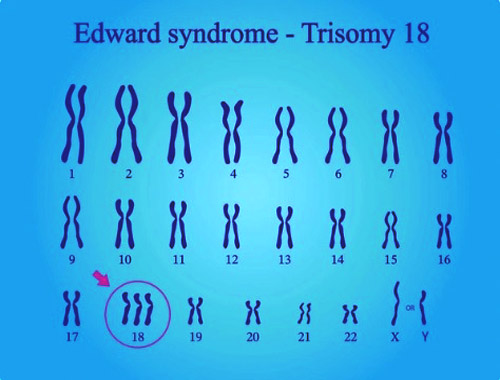
Edwards syndrome, also known as Trisomy 18, is a genetic disorder caused by the presence of a third (or part of a third) copy of chromosome 18.
Normally, humans have two copies of each chromosome, one inherited from each parent. In Edwards syndrome, there is an extra copy of chromosome 18 in all or some of the body's cells.
Here's a breakdown:
![]() Trisomy: This term refers to the presence of three copies of a chromosome instead of the usual two.
Trisomy: This term refers to the presence of three copies of a chromosome instead of the usual two.![]() Chromosome 18: This is the specific chromosome involved in Edwards syndrome.
Chromosome 18: This is the specific chromosome involved in Edwards syndrome.![]() Edwards Syndrome: This is the name of the syndrome resulting from the trisomy 18.
Edwards Syndrome: This is the name of the syndrome resulting from the trisomy 18.
Key Features and Characteristics:
Edwards syndrome affects many parts of the body, and the severity of symptoms can vary. Common characteristics include:![]() Low birth weight: Babies are often smaller than expected.
Low birth weight: Babies are often smaller than expected.![]() Distinct facial features: These can include a small head (microcephaly), a small jaw (micrognathia), a prominent back of the head (occiput), low-set ears, and a small mouth.
Distinct facial features: These can include a small head (microcephaly), a small jaw (micrognathia), a prominent back of the head (occiput), low-set ears, and a small mouth.![]() Heart defects: Heart problems are very common.
Heart defects: Heart problems are very common.![]() Brain abnormalities: Structural differences in the brain can occur.
Brain abnormalities: Structural differences in the brain can occur.![]() Kidney problems: Issues with kidney function are frequently observed.
Kidney problems: Issues with kidney function are frequently observed.![]() Physical abnormalities: Clenched fists with overlapping fingers, rocker-bottom feet, and other skeletal abnormalities are common.
Physical abnormalities: Clenched fists with overlapping fingers, rocker-bottom feet, and other skeletal abnormalities are common.![]() Developmental delays: Significant intellectual disability and developmental delays are typical.
Developmental delays: Significant intellectual disability and developmental delays are typical.
Types of Trisomy 18:![]() Full Trisomy 18: This is the most common type, where every cell in the body has the extra copy of chromosome 18.
Full Trisomy 18: This is the most common type, where every cell in the body has the extra copy of chromosome 18.![]() Mosaic Trisomy 18: In this type, only some of the body's cells have the extra chromosome. The severity of the syndrome can vary depending on the proportion of cells affected.
Mosaic Trisomy 18: In this type, only some of the body's cells have the extra chromosome. The severity of the syndrome can vary depending on the proportion of cells affected.![]() Partial Trisomy 18: This involves only a part of chromosome 18 being present in triplicate.
Partial Trisomy 18: This involves only a part of chromosome 18 being present in triplicate.
Diagnosis:
Edwards syndrome can be diagnosed:![]() Prenatally: During pregnancy, through screening tests (like blood tests and ultrasounds) and diagnostic tests (like amniocentesis or chorionic villus sampling).
Prenatally: During pregnancy, through screening tests (like blood tests and ultrasounds) and diagnostic tests (like amniocentesis or chorionic villus sampling).![]() Postnatally: After birth, based on physical examination and confirmed with a chromosome analysis (karyotype) of a blood sample.
Postnatally: After birth, based on physical examination and confirmed with a chromosome analysis (karyotype) of a blood sample.
Prognosis:
Unfortunately, Edwards syndrome is a very serious condition. Many babies with Edwards syndrome die before birth or within the first few weeks or months of life. About 5-10% survive past their first birthday. The survival rate can be slightly higher for those with mosaic trisomy 18, depending on the percentage of affected cells.
Treatment and Management:
There is no cure for Edwards syndrome. Treatment focuses on managing the symptoms and providing supportive care to improve the child's quality of life. This may involve:![]() Addressing heart defects: Surgery or medication.
Addressing heart defects: Surgery or medication.![]() Providing nutritional support: Feeding tubes may be necessary.
Providing nutritional support: Feeding tubes may be necessary.![]() Managing breathing difficulties: Oxygen therapy or other respiratory support.
Managing breathing difficulties: Oxygen therapy or other respiratory support.![]() Physical and occupational therapy: To help with development and movement.
Physical and occupational therapy: To help with development and movement.![]() Supportive care: Providing comfort and managing pain.
Supportive care: Providing comfort and managing pain.
Parental Support:
Having a child with Edwards syndrome is extremely challenging. Support groups and resources are available to help parents cope with the emotional, medical, and financial challenges involved. These resources can provide information, guidance, and a sense of community.